
Following the recent publication of European meta-analysis findings on the outcomes and overall body of evidence associated with flow diverters, NeuroNews speaks to multiple physicians from the worlds of interventional neuroradiology and neurosurgery to discuss the much-debated role these devices play in unruptured aneurysm care.
The treatment of unruptured intracranial aneurysms is a contentious topic for several reasons. The very nature of these aneurysms as non-acute—and their interventional treatment therefore being elective—continues to stimulate debate over conservative versus more proactive management strategies. And, even in instances where the latter is favoured, the various merits and pitfalls of the specific techniques available to interventionists are hotly contested too.
Despite open surgical clipping being the longest-standing procedure used to treat brain aneurysms, the turn of the last century saw coil embolisation emerge as a valid, minimally invasive option based on the findings of the ISAT randomised controlled trial—a seminal study that also paved the way for subsequent, alternative endovascular approaches. One such approach involves implanting a flow-diverting stent into a patient’s neurovasculature to channel blood flow away from and ultimately occlude their aneurysm.
The first of these flow diverters to secure major regulatory authorisations and become widely used across the globe was the Pipeline embolisation device (Medtronic), which received a European CE mark in 2008 and US Food and Drug Administration (FDA) approval in 2011. Two other families of flow-diverting stents—Surpass (Stryker) and Fred (Terumo Neuro)—have since been approved in both of these geographies, with Silk (Balt), p64/p48 (WallabyPhenox), Derivo (Acandis) and Tubridge (Microport) also subsequently cleared in Europe.
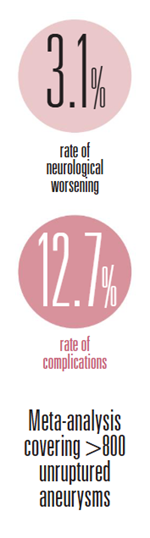
As such, flow diversion has been a fixture within brain aneurysm care for a number of years, and physicians now have a range of technologies available to them. Despite this, the clinical evidence on the appropriate role for these devices remains a subject of dispute. The most recent example of this came towards the end of 2025 when a research team led by neurosurgeon Nima Etminan (University of Heidelberg, Germany) published a meta-analysis in the European Stroke Journal assessing existing clinical data on flow diversion in unruptured aneurysms. Their conclusion reads as follows: “The literature on flow-diverting stents is methodologically weak and potentially biased by financial interests, but still shows relevant proportions of complications and post-treatment morbidity. Currently, there are no good data supporting the use of flow-diverting stents for unruptured intracranial aneurysms where standard treatment options are available.”
This damning verdict is aligned with the European Stroke Organisation’s (ESO) 2022 guidelines on the management of unruptured aneurysms, which recommend that flow diverters should only be considered “when there are no other low-risk options” for aneurysm repair—a notion that was challenged by the neurointerventional community at the time.
 The following year saw neuroradiologists Martin Bendszus and Markus Möhlenbruch—also from the University of Heidelberg—respond via an open-access letter published in the same journal. The authors take issue with the aforementioned statement that flow diversion should only be used in the absence of any other valid treatment options, arguing that the sole basis for this was a small, prematurely halted study that “goes back to the early days of the application of flow-diverting stents” and has subsequently been criticised for “severe methodological flaws”. Bendszus and Möhlenbruch also highlight a “plethora” of more recent data—both retrospective and prospective—demonstrating the “overwhelming safety and efficacy” of flow diversion in unruptured intracranial aneurysms.
The following year saw neuroradiologists Martin Bendszus and Markus Möhlenbruch—also from the University of Heidelberg—respond via an open-access letter published in the same journal. The authors take issue with the aforementioned statement that flow diversion should only be used in the absence of any other valid treatment options, arguing that the sole basis for this was a small, prematurely halted study that “goes back to the early days of the application of flow-diverting stents” and has subsequently been criticised for “severe methodological flaws”. Bendszus and Möhlenbruch also highlight a “plethora” of more recent data—both retrospective and prospective—demonstrating the “overwhelming safety and efficacy” of flow diversion in unruptured intracranial aneurysms.
Etminan and colleagues’ 2025 meta-analysis attempted to address this by providing a more comprehensive and up-to-date overview of the current evidence, but arrived at a similar conclusion to the one outlined by the ESO three years earlier.
Neurosurgeon Victor Volovici (Erasmus University Medical Center, Rotterdam, Netherlands)—who penned an accompanying editorial in the European Stroke Journal that discusses the ongoing challenges faced by flow-diversion treatments—believes “emotion” is among the main reasons why this debate continues to rage on in spite of Etminan et al’s findings.
“I think there’s a lot of emotion, especially in the endovascular world—which, to some extent, is understandable,” he tells NeuroNews. “But we need to free our minds of emotion and look at what the data are telling us in order to provide the best treatments for our patients.”
Volovici also highlights the inherent between-specialty biases underlying many of these discussions: for the most part, interventional neuroradiologists lean towards flow diversion and the other endovascular procedures they typically perform; neurosurgeons lean towards open techniques like clipping; and neurologists tend to hold a preference for avoiding interventional treatment in favour of more conservative medical management strategies.
Nevertheless—and in spite of the available data on flow diverters being “imperfect”—Volovici argues that “we should be able to see exactly what is going on, unshackle ourselves from our respective religions, and look critically at what the data are telling us”.
“For example,” he adds, “I’m a very big proponent of microsurgery—but not for every case, of course, because I’m also a proponent of thinking.”
Evidence versus experience
Across 13 studies and more than 800 unruptured aneurysms, Etminan et al’s analysis reveals a 3.1% rate of neurological worsening as well as a 12.7% complication rate at three months. Volovici also highlights prior publications showing complication rates as high as 16%, which he describes as “a significant number”, particularly given the context that many of these patients are asymptomatic and are being treated electively.
One of the major points of incongruity within this debate stems from the fact that flow-diverter treatments are extremely nuanced, requiring high degrees of skill, experience and understanding in order to maximise the likelihood of a safe and effective procedure. As such, many of the field’s most renowned neurointerventionists—particularly the flow-diversion pioneers who have been implanting these devices for well over a decade across hundreds of cases—may well be achieving much lower complication rates than those reported in last year’s meta-analysis.
“My problem with the ESO analysis is that the papers they’ve ended up with are quite niche studies that are not very reflective of standard practice”
Philipp Taussky
“Most endovascular specialists will say, ‘I do not recognise these numbers—in my practice, we do not have these complication rates’,” Volovici avers. “This is one of the issues that you can see exuding through the results of that meta-analysis. Let’s say your results with flow diverters are better than most—okay, I can live with that. But, if everybody else starts doing what you’re doing based on this, their complication rate could be as high as 16%, because the results of the procedure are so operator-dependent. This creates a problem if you then start claiming that flow diversion is best for patients.”
Perhaps, as Volovici alludes to here—and as others have called for in recent times—the modern proliferation of technologies and treatment approaches creates a need for interventional aneurysm care to be confined to larger, high-volume centres that encounter enough of these cases to develop, and maintain, the requisite capabilities to administer these therapies.
When it comes to firsthand experience, few physicians are better-placed than interventional neuroradiologist István Szikora (Semmelweis University, Budapest, Hungary) to discuss flow diverters and their appropriate usage. Szikora played a leading role in the PUFS study, which helped to establish the benefits of flow diversion, and he has also been implanting these devices since 2009.
While he admits it may not be a particularly “kind or polite” sentiment, Szikora feels that endovascular aneurysm treatments should be restricted to centres like his own that are appropriately equipped in terms of case volume, relevant expertise, availability of devices and overall infrastructure.
“But, for centres that do not have these capacities, I would very strongly recommend that they do not treat aneurysms. It’s that simple,” he continues, speaking with NeuroNews. “There are very few people who can collect sufficient experience in treating aneurysms, either surgically or endovascularly. Even with the continued growth of endovascular aneurysm treatment, there are not so many cases that people in smaller centres can collect enough experience. And, without sufficient experience, it doesn’t matter which technique you use—your results will be worse.”
Szikora goes on to note that this is especially pertinent regarding flow diversion, as these procedures can appear to be “a piece of cake” when performed by sufficiently trained, experienced operators. While the majority of flow-diverter implantations are relatively straightforward from a technical standpoint and do produce successful results, the minority of cases that go wrong provide a clear demonstration of the importance of understanding coupled with skill. An example Szikora uses is the fact that a simple, successful flow diversion may be comparable to a simple, successful coiling procedure, but flow diverters become more problematic when complications arise due to—among other factors—stents being harder to reposition and replace than coils.
Commenting that “centralisation is important” in ensuring optimal outcomes, Volovici is aligned with Szikora as well as a similar assertion made by neurologist Edgar Samaniego (University of Iowa, Iowa City, USA) in NeuroNews last year.
“Guidelines like the ones from the ESO are intended for all centres, including those that only treat 20 aneurysms each year and have nowhere near the experience levels of the leaders in the field,” Volovici adds. “It’s not realistic to expect that flow diversion will produce the same outcomes at these hospitals compared to centres treating a hundred aneurysms every year. Our expectations should be adjusted to the setting where these procedures are taking place.”
Herein lies a fundamental problem associated with these recommendations, however: their attempt to apply universal guidance on such a complex and nuanced therapy appears flawed given the many variables that flow-diverter outcomes are dependent upon. Ultimately, this can be seen to limit the recommendations’ real-world utility—especially for high-volume centres housing experienced proceduralists.
Neurosurgeon Philipp Taussky—an early adopter of flow diversion who, alongside Christopher Ogilvy at Beth Israel Deaconess Medical Center (Boston, USA), now places more than 100 of these devices annually—gives a candid take regarding the issue of treatment variability.
In his view, “no one wants to admit to this”, because modern medicine has “rightly” moved towards standardisation and homogenisation, and a multidisciplinary, collaborative approach whereby every patient in the same country—if not across the globe—should get the best treatment possible for their specific condition.
“I do think there will always be differences in brain aneurysms compared to cardiac surgery, for instance, where a bypass is always the same and valve replacements are all very similar,” Taussky tells NeuroNews. “Aneurysms are so heterogenous because of the size, location, morphology and patient anatomy. Every aneurysm is different, so the level of operator skill, experience, knowledge, setup and infrastructure will forever affect the outcomes for these patients.
“There has always been a schism in the flow-diverter world between busy practitioners who have excellent results, and other practitioners who do these procedures less commonly and struggle with higher perioperative complication rates. I do think younger physicians should spend time in busy flow-diverter centres to get a firsthand look at when and how to use these devices.
“Flow diversion also requires a completely different mindset compared to coiling or clipping, because you need to think about the diseased segment and how to remodel it rather than manipulating the aneurysm itself in order to treat it. As such, you have to think more about proximal and distal landing zones, wall apposition, and DAPT [dual antiplatelet therapy] management.”
Another factor Taussky highlights that must be considered alongside the ESO’s recommendations relates to longstanding geographic variability.
“The data are poor, and the methodologies they’re based on are not very strong, which leaves more room for interpretation—but my main comment is not that people shouldn’t use flow diversion; it’s that people should be wary and interpret the data with nuance”
Victor Volovici
“My initial reaction was that this shows the real difference between practices in Europe and the USA—and it’s been this way since flow diversion entered medical practice,” he says. “When flow diversion entered medical practice in Europe, it was not embraced at all and it was fraught with significant complications, whereas we really adopted and pushed the limits with flow diversion in the USA, and it became the first-line treatment for sidewall carotid aneurysms.”
This discrepancy is apparent within the closest US equivalent to the ESO’s recommendations: the American Heart Association (AHA) guidelines on the management of unruptured intracranial aneurysms. Having been published back in 2015—when the approach was still very much in its infancy—the only reference to flow diversion in these guidelines describes it as “a new treatment strategy that may be considered in carefully selected cases”. The AHA therefore appears to take a more lenient stance on flow diversion as compared to its European counterpart.
“I think those guidelines definitely need to be updated, and I’m sure they’re working on that,” Taussky comments. “The problem with all of these guidelines is that technical innovation—not just new devices, but management of DAPT and so on—really outpaces any of these recommendations.”
As previously outlined, the initial ESO recommendations published in 2022 were met with umbrage by much of the neurointerventional community—but has Etminan et al’s more recent attempt to synthesise existing data on flow diversion been greeted more positively?
Szikora says he “more or less accepts” the broader recommendations made by the ESO, at least to the extent that “these technologies should be used carefully”, adding that physicians “need to consider a lot of factors”—including DAPT, which is mandatory alongside flow diversion but not coiling.
“On the other hand,” he continues, “the recommendations—and the 2025 meta-analysis—are clearly coming from people who are not practising [with flow diverters]. There is a difference between very carefully reading what has been published, and actually doing what the subject of those publications is; they’re not the same thing. For instance, in this paper, there are a lot of things that are not considered at all, such as the antiplatelet protocols applied in these cases, and what kind of complications could be related to an appropriate or inappropriate antiplatelet approach. In my mind, these are very important questions—and I acknowledge that it’s very difficult to consider all of those things, but making such strong recommendations is difficult as well.
“So, will I very carefully read the recommendations and use them to decide what I should do in every single case? No, I will not.”
Taussky offers a similar perspective from across the pond. While he acknowledges that it is somewhat “unacademic” to disregard the literature in favour of one’s own experiences—and that, in general, publishing, analysing and comparing clinical data is “extremely important”—he also calls into question the evidence base for Etminan et al’s meta-analysis.
“My problem with the ESO analysis is that the papers they’ve ended up with are quite niche studies that are not very reflective of standard practice,” he notes. “Many of them include flow diverters that are obsolete and no longer available, and many of them address very niche aneurysm locations like the distal anterior cerebral artery [ACA] or the anterior choroidal artery, meaning the meta-analysis ends up in a rabbit hole that’s not reflective of general clinical practice. That’s the fundamental problem they’re facing. And it’s not clear to me from their methodology how they ended up with these papers—and they are really niche papers, many of which I’d never heard of before—instead of larger, more established series published in better journals.”
The appropriate role for flow diversion
This critique raises multiple key questions beyond the ESO guidance itself, with the most important arguably being the precise role for flow diverters in aneurysm care.
“At this point, the evidence does not suggest that the role for flow diverters is in small or medium-sized aneurysms,” Volovici says. “The evidence only supports their use in the large or giant aneurysms that they were originally made for.”
What Volovici alludes to here is the Pipeline flow diverter’s initial US FDA approval in 2011 limiting its use to patients aged ≥22 years with large or giant wide-necked aneurysms located from the petrous to the superior hypophyseal/ophthalmic segment of the internal carotid artery (ICA)—with further post-approval data from the PREMIER study later seeing its instructions for use (IFU) expanded to include adult patients with small or medium wide-necked saccular or fusiform aneurysms from the petrous ICA to the ICA terminus.
In his European Stroke Journal editorial, Volovici draws attention to the fact that nearly 90% of the 527 aneurysms included in Etminan et al’s analysis were <10mm in size, meaning “the scientific literature overwhelmingly deals with off-label indications of flow diverters”.
While Volovici is critical of this extrapolation of flow-diverter usage beyond the scope of their original purpose, Taussky points out that such a discrepancy between regulatory indications and real-world clinical practice is not uncommon in the fast-moving neurointerventional space, where innovation continues to outstrip regulation.
“It’s always been the case that flow diversion is being used in off-label situations and, frankly, it’s being used with great success in many instances—for fusiform aneurysms, dissecting aneurysms, and blister-like aneurysms,” he comments.
Meanwhile, Szikora states that, while he does often use flow diversion in larger, wider-necked aneurysms—with coiling being preferred for many smaller aneurysms—this is not the most essential driver of his chosen strategy.
“Today, there is an increasing tendency of using flow diverters for bifurcation aneurysms, and—in my opinion—that is a questionable practice, and one that I don’t follow. I have a fear that, because flow diverters are promoted so much by some physicians and by industry, it is seen as fashionable”
István Szikora
“What really matters is the morphology of the aneurysm and the anatomy of the surrounding vessels—not the size of the aneurysm itself,” he explains. “In my view, flow-diverting stents are designed to treat sidewall aneurysms, and that is very important in my decision-making. Let’s say you have a carotid artery aneurysm arising right at the origin of the ophthalmic artery—a pseudo-bifurcation situation—that is 8–9mm with a 4mm neck; I have no doubt this patient is best treated with a flow diverter. However, if you have a same-sized aneurysm in an MCA [middle cerebral artery] bifurcation, I would definitely not use a flow diverter.”
Szikora goes on to clarify that, while sidewall and ‘pseudo-bifurcation’ aneurysms are a “good indication” for a flow diverter, he typically opts for alternative approaches like coiling or intrasaccular therapy in more symmetrical, ‘true’ bifurcation aneurysms due to challenges created by the second vessel branch regarding device placement and positioning. Perforator-rich areas like the MCA and basilar artery also represent a “potential concern”, he adds.
“Today, there is an increasing tendency of using flow diverters for bifurcation aneurysms, and—in my opinion—that is a questionable practice, and one that I don’t follow,” Szikora continues. “I have a fear that, because flow diverters are promoted so much by some physicians and by industry, it is seen as fashionable. It’s also fashionable—and there’s definitely a strong push from industry here—to go into smaller and smaller vessels to treat more distal, more complicated aneurysms. I believe this is a dangerous path.”
Taussky proffers a similar level of caution; he generally avoids flow diversion in bifurcation aneurysms, and in MCA and ACA locations. However, he is critical of the ESO’s broad recommendation that flow diversion should only be used in cases where no other treatment options are deemed appropriate too.
“There are a few important things that I believe are not considered here,” he explains. “The [greatest asset] of flow diversion is that there is no recurrence—once an aneurysm is occluded, it is not going to recur. It is the only endovascular aneurysm treatment where this is the case. So, if you look at the recurrence and retreatment rates after coiling, and you are thinking about complications, you should consider complications from potential retreatments as well, and you are then calculating complications from multiple treatments rather than just one. This is not really considered in the meta-analysis, which tries to suggest that treating an unruptured aneurysm with flow diversion leads to significantly more complications, and is associated with poorer outcomes than coiling or clipping. It is a highly oversimplified approach.”
The fact this phenomenon has not been factored into the ESO’s considerations is likely due to a distinct paucity of long-term follow-up data on flow diverters and aneurysm treatments more generally—as opposed to a deliberate omission by the authors. Nonetheless, for Taussky, this is a “very important” detail, as the availability of such data would “definitely” reveal differences between coiling and flow diversion in terms of recurrence rates.
“One of the really unique characteristics of flow diversion is that occlusion rates go up over time, whereas those results get worse over time with both clipping and coiling, and that improved occlusion is not typically associated with higher complication rates,” he continues. “Another is that the treatment is curative; you have a dysplastic, diseased segment, and the aneurysm is just a reflection or a symptom of that disease. Either clipping or coiling really doesn’t address that underlying problem, whereas flow diversion—because it remodels this entire diseased segment—has a chance of curing the patient. This is also reflected in the fact that there are [almost zero] cases of recurrence in the literature.”
Where do we go now?
Even after taking into account the many nuances surrounding flow-diverter therapies, the existing body of evidence on these devices is—to say the least—imperfect.
Volovici highlights the fact that high-quality data on all aneurysm interventions, including flow diversion and other endovascular procedures, but also surgical techniques like clipping, are “really scarce”. Additionally, the lack of evidence regarding the long-term outcomes of these treatments is problematic, with many studies tending to refer to durability at one or two years despite the fact that “we are talking about lifelong bleeding risks here”.
“That remains insufficiently studied at this point, which is a severe issue,” Volovici states. “I hope that, in the future, we can have a wide-scale European registry that allows us to get into the nitty gritty of the data.”
In Volovici’s view, while investigator-led endeavours may yet improve matters, there is no major incentive for flow-diverter companies to fund large studies of products that are already approved and on the market. He also retains a level of scepticism over much of the research conducted on flow diversion to date—particularly those studies that have been driven by the companies developing these devices.
“If you say ‘trial’ in the epidemiological sense, then most people will assume you’re talking about testing a hypothesis and doing randomisation with a control group,” Volovici says. “We do have some one-arm trials, but they’re usually used when randomisation is not feasible or ethical. To me, all of the ‘trials’ of flow diverters are just prospective, multicentre, observational registries, which give you some positive results but are a long way from the evidence generated by trials of thousands of patients. I suspect they are being referred to as trials in order to create the impression that the level of evidence is higher than it actually is. It’s a very subtle marketing ploy.”
Consistently low numbers of aneurysm cases have always hindered research efforts in the neurointerventional space. Many cardiology trials are able to recruit thousands of patients when evaluating new therapies. The COATING trial—which is comparing surface-modified versus ‘uncoated’ flow diverters, and remains one of the only randomised studies of any endovascular aneurysm therapy in the 25 years since ISAT—enrolled a total of 171. Taussky notes that, as such, the unanswered questions that do exist in the world of flow diversion “are really hard to get to the bottom of”.
Additionally, the industry involvement referred to here by Volovici—and, similarly, the “financial interests” condemned previously by Etminan et al—will forever remain a complex issue, according to Taussky. In his view, one of the strongest aspects of the 2025 analysis is the fact that it flags up the enduring role played by industry, as this is an especially pertinent topic in the flow-diverter space. When it comes to retrospective case series, for example, Taussky feels physicians should be “very careful” and mindful of possible “underlying agendas”. However, he also warns against being too dismissive of studies like PUFS, PREMIER and SCENT that laid the groundwork for Medtronic and Stryker to gain regulatory approvals for their flow diverters.
“It may lower the bar for scepticism, but the fact a study is industry-sponsored does not automatically mean the data are poor, or biased,” Taussky comments. “And, we have to acknowledge that this innovation is industry-driven and, without industry, we wouldn’t have any of these studies, and we wouldn’t have any of the modern devices we see in [neurointerventional care] as well as cardiology and oncology.
“It’s a complicated discussion; we’re grateful to industry for advancing the management of these disease states, and advancements have been incredible, but we also need to make sure that strong, unbiased data get published.”
While industry input and promotion regarding flow diverters may have an impact “to some extent”, Szikora’s advice to other physicians wishing to mitigate these effects is to have a strong understanding—via clinical evidence and literature—of the technologies at hand, and maintain relationships with sales representatives but, more importantly, with engineers in order to see the “true value” of new devices.
“There are maybe six or seven flow diverters currently being produced by different companies, and each company has some arguments about why its flow diverter is better than the others—but, if you look at the literature and read the results, there are basically no differences,” he says. “So, if one device is working well in my hands, should I try another device for the same purpose and the same pathology just for the sake of trying it? I don’t do that. In order to switch from one product to another, I need to be convinced that there’s something missing from the one I’m used to. That would be my recommendation: to fully understand what you want to fix and whether it will potentially be improved with a different device.”
Putting the potential challenges created by industry-driven biases to one side, the lack of high-level evidence on flow diversion—particularly longer-term follow-up data—remains a point of contention. The final message delivered by Etminan et al in the conclusion of their meta-analysis is as follows: “Randomised controlled trials are needed to compare safety, efficacy and durability between flow-diverting stents, and coiling or clipping.”
However, Taussky voices reservations regarding how feasible trials of this kind are likely to be, while Szikora harbours doubts over the actual value their results would hold.
“One problem is that I don’t think patients are going to agree to randomisation; another is the question of who is going to pay for these trials,” Taussky comments. “And, by the time many of these studies are finished, the devices will already be outdated, because you need at least 3–5 years to run these trials and have long-term follow-up—and, by that time, you will already have had one or maybe even two new generations of flow diverters. I don’t think randomisation is ever going to happen in this space.”
“In my view, there is no comparison between coiling and flow diversion,” Szikora adds. “Of course, there are aneurysms in which I use a flow diverter plus coils but, outside of that, there are many aneurysms I would not hesitate to treat with coils and many I would not hesitate to treat with flow diversion. So, in my practice, I could not compare them directly, because I use them for different types of aneurysms.”
This concept likely precludes any future randomisation between coiling—the closest thing to a standard of care in contemporary endovascular aneurysm treatment—and flow diversion. The same line of thinking can also be seen when looking back to the early days of flow diversion as, in the PUFS study, it was a prerequisite that enrolled aneurysms had already been deemed untreatable with coils.
 “I don’t think the data are sufficient, but when can we say that data are sufficient?” Szikora continues. “The major challenge for clinical research—particularly in our field—is to select comparable patient groups across a large number of centres. A good example of us getting this wrong was the ARUBA trial, which compiled data on any kind of brain AVM [arteriovenous malformation] with the only selection criteria being ‘unruptured’. We know that there are so many types of AVMs that such a comparison was pretty much useless.
“I don’t think the data are sufficient, but when can we say that data are sufficient?” Szikora continues. “The major challenge for clinical research—particularly in our field—is to select comparable patient groups across a large number of centres. A good example of us getting this wrong was the ARUBA trial, which compiled data on any kind of brain AVM [arteriovenous malformation] with the only selection criteria being ‘unruptured’. We know that there are so many types of AVMs that such a comparison was pretty much useless.
“The same problem exists with aneurysms. I would say, if we want to understand the true value of flow diversion, we should look at a large number of flow-diverter cases in infra/supraclinoid carotid artery aneurysms, or in basilar or distal vertebral artery aneurysms, or potentially the sensitive issue of more distal aneurysms in the MCA. These groups should be differentiated, because they are completely different stories that cannot be compared to one another. However, this type of research is something that could only be provided by a very strong international cooperation.”
Recently, the neurointerventional community has attempted to take steps in this direction. A new guideline on flow diverters—endorsed by multiple groups including the European Society of Minimally Invasive Neurological Therapy (ESMINT) and Society of NeuroInterventional Surgery (SNIS)—was also published in 2025, concluding that, “when widely applied, standardisation of methods of measuring and reporting outcomes will help to harmonise the assessment of treatment outcomes in clinical studies, help facilitate communication of results among specialists, and help enable research and development to focus on specific aspects of flow-diversion techniques and technology”.
With randomised trials—for various reasons—appearing very unlikely, Volovici echoes these sentiments, emphasising the pivotal role for multidisciplinary, collaborative decision-making and more comprehensive follow-up protocols in ensuring the highest possible standards of both clinical care and data on unruptured aneurysms. He recommends that, in cases adjudged to be amenable to endovascular and surgical options alike, the patient should be counselled by each of the relevant specialists.
“That’s how it should be,” he explains. “None of us feel like someone else is stealing our cases—there’s enough for all of us, and we don’t have any turf wars. That’s the only way that you can really get this going, aside from the US system where people are dual-trained.”
Even more recently, in June 2026, both Volovici and Taussky were co-authors on another European Stroke Journal publication outlining new measures on studying the safety, efficacy and durability of intracranial aneurysm devices, including the appropriate role for randomised controlled trials and registries as well as the need for clarity on indications and standardised definitions.
“Another essential point is that people should follow up these patients,” Volovici concludes. “Even if they have been treated microsurgically and their aneurysm has completely disappeared on imaging, I still do a six-month MRI [magnetic resonance imaging], neuropsychological assessments, and one- and two-year follow-up. This benchmarking is important. It’s the only way we’ll ever get better data compared to what we have right now, and the only way for us to confirm that the things we assume about post-treatment outcomes are correct as well.
“The data are poor, and the methodologies they’re based on are not very strong, which leaves more room for interpretation—but my main comment is not that people shouldn’t use flow diversion; it’s that people should be wary and interpret the data with nuance.”










