With mechanical thrombectomy now long-established in ischaemic stroke care, its continued expansion as well as further improvements in associated outcomes moving forward will be more incremental compared to the revolutionary progress seen over the past decade—with larger clinical trials and more proactive treatment paradigms likely being required to drive this forward. These were among the salient points conveyed by Raul Nogueira (University of Pittsburgh Medical Center, Pittsburgh, USA) via a recent presentation at the 2026 LINNC Paris course (1–3 June, Paris, France).
“One of the most misunderstood topics in our field is this idea that people don’t benefit from thrombectomy—we need to understand the difference between benefit and good outcomes,” Nogueira asserted. “How do we improve outcomes in patients who still don’t benefit? The answer is to do more thrombectomies. There are other factors, but the main reason we are not seeing a greater benefit is that we are undertreating with thrombectomy. That is a critical message.”
According to Nogueira, many operators use magnetic resonance (MR) or computed tomography (CT) perfusion imaging to estimate how likely a given patient is to derive benefit from thrombectomy treatment. However, while these tools may be suitable for prognostication, they are—at present—“incapable” of reliably predicting who will benefit from these interventions.
“Most imaging biomarkers are predictors of outcome rather treatment effect modifiers. Therefore, these techniques should not be used primarily to exclude patients from thrombectomy,” Nogueira clarified.
To demonstrate this point, he cited data from the JURaSSiC study, in which 111 expert clinicians were asked to predict the probability of various outcomes across five ischaemic stroke case scenarios. Some 48% were unable to accurately predict the probability of the primary outcome—a modified Rankin scale (mRS) score ≥3—in any of the five cases, and none accurately predicted the outcomes of all five scenarios.
“This is worse than tossing a coin—but this is what we are doing in our daily practice,” Nogueira commented, also noting that more recent studies have revealed similar trends. “We are not good at predicting outcomes and, if we cannot predict, we cannot assume; when in doubt, we must treat [with thrombectomy].”
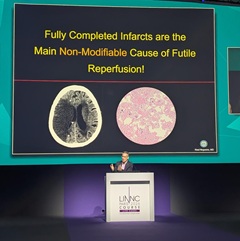
Another key problem, Nogueira continued, is that physicians fail to distinguish between a ‘good outcome’ and overall clinical benefit, often falsely attributing mRS scores >2 to the phenomenon of futile reperfusion.
“We have this paradigm of angiographic-clinical mismatch,” he explained. “People will say that we open the vessel up 90% of the time but only 50% of patients do well—meaning they achieve functional independence [mRS 0–2]—and this has been defined as futile reperfusion, but that’s not actually true. We are mistakenly labelling any case without a good outcome as ‘futile’, even if they experience a better outcome than they would’ve had without thrombectomy.”
Nogueira posited that the idea of futile reperfusion must be revisited, also criticising the dichotomisation whereby thrombectomy is considered to have been successful if a patient achieves an mRS score of 0–2 versus unsuccessful if their mRS score is 3–6. In his view, more emphasis should be placed on mRS ordinal shift analyses and utility-weighted scoring, which go some way to avoiding this oversimplification.
“Sometimes, a good outcome is just not possible, but there may still be a benefit in terms of shifting patients towards reduced disability,” he added. “The absence of a good outcome is not equal to futile reperfusion, and the goal should not be ‘good outcomes’ but, rather, ‘better outcomes’—meaning any functional improvement.
“Part of the problem is also a lack of understanding of the difference between predictors of outcomes and treatment-effect modifiers. We consider older ages, late time windows and large cores to be predictors of a worse outcome. But, if you compare similarly treated patients, with similar age, time and size of stroke, none of these things nullify treatment effect, so we shouldn’t be using them to exclude people from thrombectomy.”
Subsequently, Nogueira touched on the ‘denominator fallacy’, which, in his view, demonstrates “how egocentric—versus patient-centric—medicine can be”. Using the EXTEND-IA randomised trial as an example, he noted that the overly selective use of CT perfusion imaging has been shown to result in a high rate (70%) of 90-day mRS 0–2 and a number needed to treat (NNT) of 3 among patients receiving thrombectomy, while more inclusive selection via non-contrast CT means a greater number of patients undergo the procedure, leading to a lower average rate (35%) of mRS 0–2 and an NNT of 5 across this broader cohort.
“But, we can’t forget that our duty is not only to the patients we operate on, but to all the patients we consider for treatment,” Nogueira commented, highlighting the fact that, across all patients imaged as potential thrombectomy candidates in the previous example, over-selection led to 10% experiencing benefits compared to 16% when more inclusive criteria were used. “Being more selective means my personal outcomes will look better, but it’s not about me; it’s about patients. And, right now, we are leaving a lot of them behind.”
On the topic of large-core ischaemic strokes, Nogueira stated that—while a possible ceiling effect in core volumes >150ml was revealed by the latest data from the ATLAS meta-analysis—the procedure has consistently demonstrated benefits across the majority of patients with these more severe infarcts. He also posited that the density of these infarcts—as measured by net water uptake—in addition to the volume, appears to be important in determining whether damage to the brain can be halted and reversed via a thrombectomy procedure, as per imaging data from the SELECT2 and TENSION trials. As such, Nogueira added, core volumes alone should not be used to exclude patients from these treatments.
Similarly, the relevance of an individual patient’s frailty and biological age, as opposed to merely chronological age, is also becoming increasingly recognised, according to Nogueira.
He went on to acknowledge, however, that some patients do genuinely experience poorer post-thrombectomy outcomes despite initially appearing to be good candidates for the procedure.
One driver of this is believed to be reperfusion injury, with Nogueira noting its underlying causes—including excitotoxicity, oxidative stress and inflammation—represent potential therapeutic targets. Usage of neuroprotection as an adjunct to thrombectomy has demonstrated promise here; Nogueira highlighted positive findings from OPENS-2—a randomised trial published last year in The Lancet, which found that the “simple” approach of normobaric oxygen therapy can safely improve outcomes in patients treated endovascularly. He also drew attention to intra-arterial brain cooling during thrombectomy procedures, remote ischaemic conditioning using standard blood pressure cuffs, and numerous drug candidates, that have all produced positive signals in clinical studies.
Suboptimal thrombectomy outcomes have also been attributed to the ‘no-reflow’ phenomenon, whereby the procedure successfully restores blood flow within the ‘macro-circulation’, but smaller occlusions remain within the brain’s ‘micro-circulation’. On this front, Nogueira highlighted recent evidence from the CHOICE2 trial indicating that giving alteplase after thrombectomy may boost outcomes, but added that new thrombolysis solutions that target more of a blood clot’s constituent parts, including platelets, Von Willebrand factor (vWF), neutrophil extracellular traps (NETs) and DNA—as opposed to just fibrin—may be needed too.
“We need to understand that the low-hanging fruit is gone,” Nogueira concluded. “The trials we did in the past compared thrombectomy to medical management; now, we are in an age of comparing thrombectomy plus something else versus thrombectomy alone. We are going to see more modest, incremental benefits, and what we consider to be a minimal clinically important difference will be in the low single digits, so we’re going to need much bigger trials.”











