In the ANSWER (Adjunctive neurovascular support of wide-neck aneurysm embolization and reconstruction) study of the PulseRider device (Pulsar Vascular), enrolment, 30-day and 180-day follow-up are complete for all 34 patients. At the moment, 365-day follow-up on eight patients is complete, and investigators are in the process of collecting these data on the remaining patients; which should be complete by the end of the year. Now, NeuroNews speaks to principal investigator Alejandro Spiotta (Medical University of South Carolina, USA) about his experience.
What is the purpose of the ANSWER study?
The ANSWER trial was designated as a Humanitarian Device Exemption (HDE) to prove safety and probable benefit of the PulseRider in the treatment of patients with wide-neck aneurysms at a bifurcation of the internal carotid terminus or the basilar artery. It is a multicentre, prospective, non-randomised, single-arm study that was carried out with Institutional Review Board approvals at 10 clinical sites in the USA.
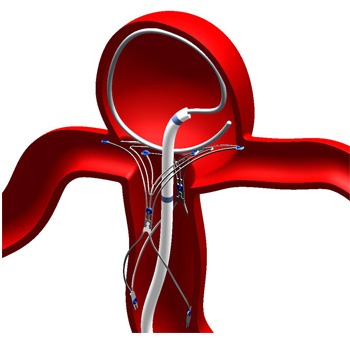
What is unique about the PulseRider device?
The PulseRider is a self-expanding, nitinol implant designed to act as a scaffold to retain coils in broad neck aneurysms. The device is available in different diameters for the parent vessel size and two arch widths to address the aneurysm neck dimension. The device is also available in two configurations, a “T” and a “Y” to best accommodate the geometry of the aneurysm and the daughter vessels. The placement is versatile in that the PulseRider can be placed across the neck of the aneurysm in the daughter vessels, in the aneurysm or in a hybrid fashion with one arch of the device in a daughter vessel and the other arch in the aneurysm. There are eight radiopaque markers on the PulseRider to aid the operator in positioning it, however, the PulseRider is fully retrievable and can be repositioned and torqued to fit the relevant anatomy. The device design has significantly less metal than a conventional stent with the majority of the surface area coverage concentrated at the aneurysm neck.
What types of aneurysms have been treated in the study?
In the ANSWER study we were limited to carotid terminus and basilar aneurysms due to the HDE in the USA.
What results have you recorded so far?
There were three primary endpoints that included safety, technical success and rate of aneurysm occlusion. In the study all of the primary endpoints were met; there were no deaths or stroke in downstream territory to 180-days post-procedure that were attributed to the device or procedure. The device was accurately deployed at the target aneurysm and successfully detached in 34/34 (100%) of the cases. Angiographic evaluation at 180-days, using the Raymond classification, was 87.9% Raymond I and II combined which was adjudicated by a blinded core lab. Also of note, related to angiographic evaluations, there has not been any migration of the device although there was one (2.9%) instance of <50% stenosis in a branch vessel at the 180-day angiogram.
What are the next steps in the study?
We will continue to collect data and do the analyses on the 365-day follow-up as it becomes available. When the data analysis is finalised this will be published. There are also preparations underway for the design of a study for a Premarket Approval to address all territories of the brain.
What have you learned about using the PulseRider device in the ANSWER study?
Although the data is still somewhat limited (only 34 patients), we believe PulseRider will be comparable when compared to stent-coiling. There should be sufficient scaffolding for neoendothelialisation to occur to achieve a durable cure. While some physicians have advocated flow diversion to be used at bifurcations to prevent recurrences, jailing of daughter branches and potential perforator occlusions may limit their safety profile.
Once approved in the USA, how do you think PulseRider will change current practice?
ANSWER provides prospective evidence that the safety profile of PulseRider is acceptable and that probable benefit to patients with broad-necked, bifurcation aneurysms is satisfactory. These aneurysms are very challenging and this new device and the results of the study suggest that it will be a useful addition to our armamentarium when treating this patient population.










