
COVID-19 represents a global challenge that has exposed the USA’s fragmented public healthcare system, writes Demetrius Lopes. Here, he details Chicago’s action plan in response to the crisis, appropriately named, “Stroke Network on Steroids”, due to the speed and magnitude of what has been implemented over the past few weeks.
As stroke experts and leaders in our field, it is critical that we can still provide stroke care to patients in need during the COVID-19 crisis. Our role is to advocate for patients with cerebrovascular disease, keep team members safe, and align our efforts with the broader public health system response. In an effort to answer this question, I was asked to share my views and actions put into place early on in response to the crisis in Chicago.
The real issue
The COVID-19 pandemic started in late 2019 in China. By March 2020 it seemed inevitable that Chicago was going to get hit early with daily reported cases on the rise. Not much was in place to control the spread with a rapid surge of acutely ill patients. There was a lack of testing capabilities, concern for supplies and equipment, and the directions from local and national level government leaders were inconsistent.
Healthcare in the USA has many positive attributes; however, the coordination of care is not one of them. The pandemic has put the spotlight on our fragmented healthcare system creating competition and mixed messages during a time when collaborative and coordinated efforts are crucial.
For everyone involved in coordination of acute stroke care in the USA, this isn’t “news.” That is not to say coordinated efforts in stroke care are fully in proportion to those efforts required for the COVID pandemic, but an understanding of barriers at the larger public health level is a reality we are already familiar with for acute stroke patients.
A call to arms
I am very thankful to our colleagues from China and Europe, who early on shared their experiences with us. We understood that any action plan had to address:
- Bed availability in the intensive care unit (ICU) and ventilator supply
- Health care team safety
- Screening, workflow, and resource allocation
With this information at hand, we prepared our response to this extraordinary situation.
The Plan: “Stroke network on steroids”
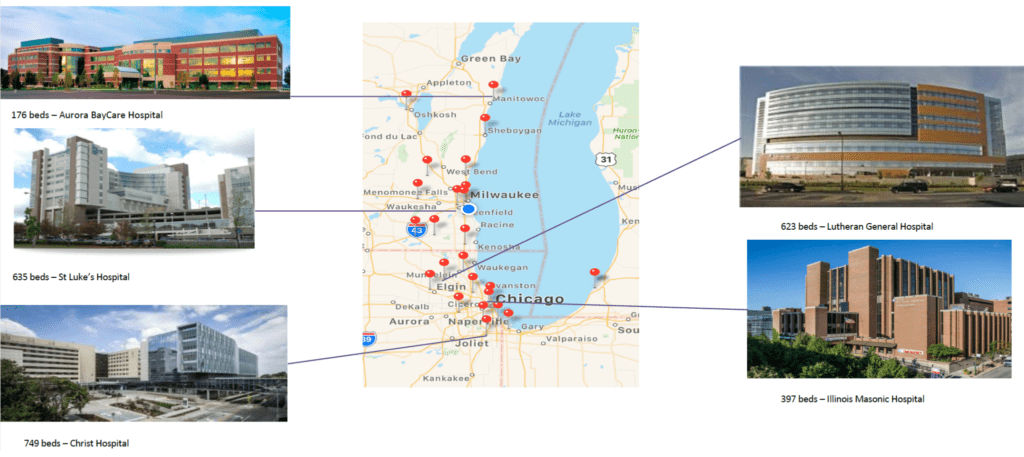
AdvocateAurora Health (AAH) is one of the largest healthcare systems in the USA. Our team coordinates stroke care in 27 hospitals in the densely populated area between Chicago and Milwaukee spanning from north Wisconsin to southern Illinois. We have five comprehensive stroke centers and one thrombectomy-ready hospital (11 interventional surgeons team), as well as many stroke-ready triage sites.
AAH began an early system-wide response creating a system incident command center that guided each of the individual site’s incident command with communication, tools, and resources for the AAH healthcare network. Advocate Aurora Stroke Network (AASN) was established before the pandemic, and we used this platform to launch our coordinated cerebrovascular care during the COVID 19 pandemic. Recognising the current focus of care is on the COVID-19 patients, we quickly understood we needed to provide our stroke programme site leaders with alternative workflows and resources to be able to continue to provide stroke care to patients presenting with stroke during the surge. Because of the magnitude of impact that the COVID crisis has placed on typical stroke care, and speed required for planning, we called this “Stroke Network on Steroids”.
Step one: Assess current status, communication tools and education
- Stop all elective cases and limit outpatient visits
Suspending elective procedures early for patients with non-emergent problems aids in reducing demand on personal protection equipment (PPE) supply and staff utilisation.
- Review of current staffing models
A review of current staffing schedules of all team members was completed. Our goal was to minimise team member exposure through a re-design of service coverage by assigning one on call provider for an entire week with all other providers to stay at home. We did this for neurosurgery, neurointerventional and our advanced practice provider teams to limit the risk of exposure.
- Create a communication line
We started by engaging all our team members (stroke coordinators, nurses, technologists, physicians, service line administrators, advanced practice providers) throughout the system. Everyone shared their thoughts and had the opportunity to ask questions on how to stay safe and be best prepared to treat patients during this period. A daily stroke system debriefing call was established. This brief call allowed for system leaders to support site specific issues and to track number of stroke patients in the system and potential gaps in care.
- Develop Assessment and Management Guidelines
With a shortage of available testing, and emerging reports documenting hypercoagulability and possibly independent neurological symptoms arising from the infection, we assume that all patients are potential COVID-19 positive if they cannot communicate or their history is not available. We created a system guideline for stroke (ischemic and hemorrhagic) assessment that provided recommendations for medical and surgical treatment pathways. This guideline for cerebrovascular intervention addressed issues of PPE, airway management, team member safety, and exposure and recovery of patients outside the normal ICU environment. For post-stroke care we focused on bed availability, staffing ratios, and educational needs.
We began using telestroke/telemedicine consultations for all acute stroke evaluations. Similar technology is also being used for outpatient appointments that did not require in person care (e.g. symptom checks). This successfully minimised the exposure of our team and increased patient access. Post-operative visits, such as those to manage sutures and wounds are more challenging to accommodate remotely and require prescreening measures performed before an in-person visit is possible.
Finally, we prepared a tiered response plan for acute stroke presentations treated with thrombolytics or thrombectomy that detailed patient placement in relation to the COVID surge constraint:
1st level (ICU capacity not reached): Continue to follow the same approved indications for treatment and disposition per our pre-existing protocols
2nd level (ICU beds at capacity): Patients will be sent to non-ICU beds but neuro floors with neuro nurses
3rd level: Patient will be sent to any available bed with general nurses (crash course in neuro)
4th level: Patient will need to be transferred to another AAH site due to lack of any available bed
5th level: Transfer patient to a non-AAH hospital
For the sites currently designated as “stroke-ready,” additional triage planning has been discussed, in the event the COVID surge prevents ability to transfer to a receiving hospital either within or outside our system. In this exceptional scenario, telemedicine will be utilised to provide the specialty consulting services not available locally for patients primarily requiring medical treatments.
Step two: Monitor development of pandemic and resource allocation as needed
Monitoring of stroke patients across the AAH stroke network is achieved through a daily debriefing call. This call allows for site and system leaders to be kept abreast of bed availability issues, site-specific emergency department surge, and volumes of stroke and COVID patients at each site. These are very fluid numbers but allow for our teams to have daily discussions for alternative options. This also helps to gauge the current tiered level of care our stroke patients are receiving.
Our centralised patient command centre (PCC) is responsible for all transfers and bed assignments across the network. Working with the PCC, we can safely assign patients with cerebrovascular disease to the closest hospital with bed availability that is capable of proving the necessary level of care.
The daily monitoring of stroke volume, number of interventions, bed availability, and the health status of the teams assist us to best use resources and increase safety to our patients in this very dynamic environment.

Step three: Coordinate a response with the local teams
It appeared crucial to “rally the troops” and bring all regional players together to share information on lessons learnt to provide safe care to patients and to keep our teams safe. In response to this need, the Chicago area neurointerventional teams connected on a chat to form the Chicago Stroke Alliance. This chat allows us to share knowledge and discuss COVID stroke-related issues. We hope that this connection will help us coordinate our resources and patient care when we are on the apex of the pandemic curve and resources become tighter for everyone.
We are facing a global challenge that has exposed our fragmented public healthcare system. It is important to be clear that there is no correct roadmap to navigate this difficult time. We hope that our approach can help you to organise a response to this pandemic in your region. As cerebrovascular specialists, our skill-set and knowledge places us in the best position to advocate for the care of our patients and protection of our teams.

Demetrius Lopes is a cerebrovascular neurosurgeon specialising in neuroendovascular therapy. At Advocate Health, he serves as medical director of the cerebrovascular and neuroendovascular programme and is co-director of their stroke programme.
Thomas J Wolfe, who reviewed the article, is an endovascular neurologist. At Aurora Health, he serves as a medical director for neuroendovascular and stroke programmes.






